The Dystonia Europe Board decided that this year our annual conference day would be held online using zoom. We used this method during the covid restrictions and not only did it work really well it was also a great deal cheaper than a face to face meeting.
We all still prefer face to face meetings but in these days of ever increasing costs we thought it was important to save money by hosting the event online, of course it also saves our members money on travel and accommodation.
We had a couple of practice runs with Edwige, our president and webinar expert, so she could sort out any problems before the big day.
The day began at 10am Central European Time with an introduction from Edwige and our volunteer moderator Rachel. We met Rachel a few years ago when we employed her to moderate our conference in London.
She was really good at keeping everything flowing and to time and she was so impressed with our work that she had moderated every Dystonia Europe (DE) conference since and not charged us!
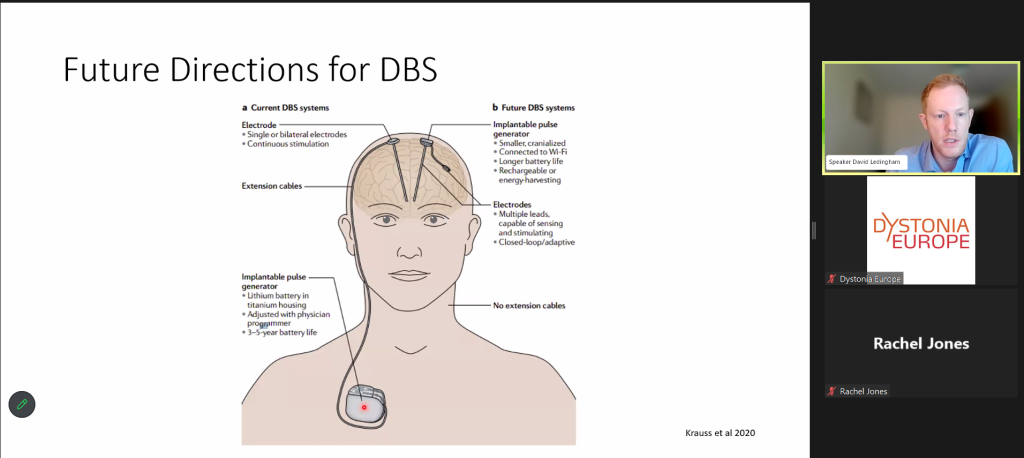
Once the introductions were done our first speaker was Dr D Ledingham, a consultant neurologist in my home town of Newcastle upon Tyne, England. Dr Ledinham spoke about his work with Deep Brain Stimulation (DBS) patients and began by explaining that DBS can help several different conditions and many thousands of people have had the procedure.
DBS has been performed for about 30 years but the idea of it has been around for much longer than that.
The procedure can be done with the patient awake or asleep depending what the surgeon prefers. In Newcastle where Dr Ledingham is based the surgery is done under general anaesthetic. For this method the location of the electrodes is thoroughly researched and mapped before the surgery begins, then the surgeon knows exactly where to place them.
Surgeons who prefer their patient to be awake use patient reactions to determine the correct placement of electrodes.
The stimulator is usually placed in the chest wall and the electrodes run up the neck to the required place in the brain. In the early days batteries did not last long however, the batteries are getting smaller and are rechargeable by the user so no need for frequent visits to hospital to get batteries changed. They do need to be changed eventually and nowadays can last 15 years, maybe longer. Dr Ledingham explained that the patient may not see a difference in their condition immediately, they are usually recalled to hospital about 1 month after surgery for a 2 hour appointment where the level of stimulation will be set and adjusted as necessary. It can take a few appointments to get the level right but the best outcome is generally between 6 and 12 months after the operation.
Technology is improving the design of the stimulators and an adaptive stimulator has recently been developed for patients with Parkinsons. This type of stimulator detects the faulty signals from the brain and adjusts the level of stimulation instantly to counteract the faulty signal.
Before a patient is approved for DBS they have several tests and assessments including a Magnetic Resonance
Imaging (MRI) scan, a neuropsychological assessment and an assessment of how it would improve their quality of life etc.
Dr Ledingham then took lots of questions, too many to list here but a lot of them were about recovery time and Dr Ledingham told us the patient would be in hospital only 1 -2 days and recover at home in about 2 weeks. A really interesting presentation on DBS which prompted lots of questions!
Next up was Dr Stavros Tsagkaris, who is this years David Marsden Award (DMA) winner. He presented the paper which won him the award and I have to be honest and say it was a bit too technical for me and I didn’t understand it all. Please forgive me if I get this wrong but my understanding was that he tested the glucose uptake (also known as metabolism) in children with dystonia. He found some correlation with hypometabolism and hypermetabolism and their dystonia. Dystonia has so far been thought to be a problem in the basal ganglia but Dr Tsagkaris’ study has shown that it is a problem in other parts of the brain and there were some common results in different types of genetic dystonia.
His results will give the medical world a better understanding of the pathophysiology of dystonia and this could lead to better targeted treatment. Another really good presentation.
We then went into a break for 30 minutes or so, time to refresh my coffee and use the bathroom. During the break Edwige played a short film that has been made of the Cervical Dystonia Patient Journey. The actress playing the part of the patient has become a friend of DE since she worked with Monika, our executive director on a short play she performed about dystonia. She portrays the condition really well and has obviously got a deep understanding of what happens to dystonia patients when they are first diagnosed, or even before diagnosis which for some of us took a long time. This film covered that journey so well that it brought tears to my eyes. I could connect with every part of the journey even though it wasn’t identical to my own journey it still brought many memories back of how hard it was in the early days. The film then went on to show that with the correct treatment we can get our lives back, for some of us that life is a little bit different to before but is just as fulfilling and enjoyable.
The next presentation was by a Dysphonia ENT specialist from Norway called Dr Jen Oyvind Loven.
Dr Loven gave a really good and concise description of dystonia. I know we probably all know exactly what
dystonia is but I always find it reassuring to hear a medical professional describe it so well.
He explained that in dysphonia the laryngeal muscles will either close, adduction, or open, abduction.
Adduction is used normally to speak and abduction allows you to breathe. He showed us a video of someone without dysphonia who could talk normally and someone with dysphonia who could only whisper or had a hoarse voice. The voice can also be jerky and sound like groaning. Lots of different types of treatment have been tried over the years including, speech therapy, psychotherapy, nerves to vocal cords severed but nothing was really successful until in the 1980s a Dr called Blitzer treated dysphonia with botulinum toxin. This was the Dr who trained Dr Loven, so he learned from the best!
Dr Loven now treats up to 200 dysphonia patients with botulinum toxin and gets best results with patients who have primary dysphonia. Their treatment is successful for around 3 to 4 months when their injections are repeated. In all the time he has been treating dysphonia he has only seen 8 patients have spontaneous remission.
He did agree with many other dystonia specialists that stress makes the condition worse and I think we can all empathise with that!
Dr Loven recommended that patients in Norway should see an ENT specialist who will then refer them to one of only 3 treatment centres in Norway. Currently there are around 300 dysphonia patients in Norway and 67% of them are female.

Jens Øyvind Loven
Rachel thanked Dr Loven for his excellent presentation and it was time to move on to Dr Dressler.
Dr Dressler is from the Medical School in Hanover, Germany but he did his presentation from somewhere in Japan and for him it was the middle of the night! We are very grateful that he agreed to do his presentation.
He has worked on stress induced dystonia for around 40 years and recently produced scientific data on the subject.
Until then the evidence of stress induced dystonia was all anecdotal. He asked us to understand that he is not talking about psychogenic or functional dystonia but dystonia induced by very severe stress. Dr Dressler took us through the scientific parameters used to select the nts for the study. He explained some of
the stressful situations his patients had experienced, such as being a refugee from a troubled country, being a prison inmate, severe physical trauma to name a few. All patients selected had rapid onset dystonia and all showed robust improvement with treatment. He found solid evidence of a correlation between excessive stress and presentation of dystonia.
100 patients took part in his study and all had rapid onset dystonia with symptoms much more severe than idiopathic or secondary dystonia.
All the patients experienced a reduction in spasms/symptoms when their stressful situation was resolved. However most of them still needed to have treatment with botulinum toxin.
I found this study very interesting. I think most of you will agree that stress makes dystonia worse, but I hadn’t realised that there was a now recognised type of dystonia which was induced by extreme stress.
Dr Dressler took a few questions and then left, I hope he managed to get some sleep!
Next up was Johanna Blom, a physiotherapist from Sweden with 17 years experience of treating Cervical Dystonia.
Johanna explained the importance of physio for dystonia and that it can retrain the brain to help with pain and spasms. Physiotherapy can be used to activate the opposite muscle directions in dystonia patients which can help to reduce the severity of the spasms and therefore the pain.
She impressed upon us how important it is for the patient to be dedicated to keeping up the subscribed exercises each day. This repetition is what is required in order to retrain the brain.
Johanna with support from Dystonia Europe, Eelco Uytterhoeven and Boston Scientific Foundation Europe (BSFE) has developed an extensive database of physiotherapy exercises for Cervical Dystonia patients.
The online platform has 115 exercises so far, some of which are animated. Professional physiotherapists need to register and then they can have free access to the platform. Then when they have a dystonia patient they can create an individual programme of exercises for each patient, they then give their patient an access code for them to access their own tailored programme.
Currently Johanna has 428 physiotherapists from 27 different countries and so far over 600 individual programmes have been created!

Physiotherapist Johanna Blom
Johanna is determined to increase the number of physiotherapists who can treat dystonia around Europe and beyond. I think she has already made a difference and I am personally grateful to her, without her platform I would not be able to have physiotherapy.
Last but by no means least was Prof Jens Volkman with an update on his research. Prof Volkman has been doing research into the genetics of dystonia and why some people with the dystonia genes will not develop the condition.
Prof Volkman explained that 70% of patients with the faulty genes will develop dystonia. There is often a trigger such as physical trauma or overuse. Writers’ cramps and musicians’ dystonia are both caused by many repetitive movements.
Also brain lesions can trigger dystonia. When a patient has the faulty gene they will have a predisposition to developing dystonia due to environmental factors. Prof Volkman was helped by a consortium of people including our very own Monika Benson. In order for them to explore the disease mechanisms they used mice who had been given the faulty gene.
They observed that the mice without any environmental trigger did not develop dystonia, however, the mice who developed overuse injuries did develop dystonia. They also performed DBS on mice trying different electrode placement and analysed the results.
They then did some video analysis of the success of DBS on cervical dystonia patients and showed that those with a tremor had a better result than those with a fixed head position. In summary the team found that dystonia has multiple disease causes but one common network dysfunction.
Their new rodent model is allowing them to study the interaction between genetic causes and environmental causes. They are also developing a new analysis method for the objective measurement of dystonia.
In question time Prof Volkman told us that there have been some studies into non-invasive brain stimulation but it will be at least 4 years before this is properly understood.
I must admit that I didn’t understand all of this presentation so I apologise if I have not understood correctly, but the main thing that I took from this presentation was that we need to understand why only 70% of people with the faulty gene develop dystonia. Wouldn’t it be great if that was fully understood? What have those people got that we haven’t? If that could be bottled it could be used to treat or cure dystonia or even prevent it from happening in the first place!
I suspect that is a pipe dream though, we all know that currently there is no cure, but it is heartening to learn that so much research is being done and one day we may all benefit.
Our moderator Rachel thanked everyone for attending and asking so many questions, and Edwige, our president, also thanked everyone for listening and of course they both thanked all our speakers for giving up their valuable time to speak to Dystonia Europe, members and friends.
I hope you all enjoyed the conference too but don’t worry if you missed it. Each presentation will be on our youtube channel very soon.
Take care everyone.
Gill Ainsley
Secretary and Vice President
Dystonia Europe

